I. Table of Contents
A. Elimination of Forced
"Treatment."
B. Public Awareness
About the Lack of Effectiveness and Extreme Harm of Treatments
(1)
Public Awareness that There is No Evidence Supporting the Broken Brain Theory of
Mental Illness
C. Availability of Truly
Helpful Alternatives
VII.
Psychiatry’s Vulnerabilities
II. Purpose and Summary
The purpose of this paper is to provoke discussion around how to organize the grass roots efforts for human rights in mental health by laying out a potential approach. There are two central themes of this paper. The first is that while an attack on human/civil rights abuses could be viewed primarily as a legal issue, success hinges on three key elements:
(1) Public Education,
(2) the Availability of Alternatives, and
(3) Legal efforts,
to which can naturally be added the Action Conference's two additional tracks,
(4) Government Relations and
(5) International.
Government is an omnipresent force in coercive psychiatry as well as controlling what services will be provided and establishes the legal framework. It clearly justifies a focused effort as well. Similarly, with the rise in forced psychiatry around the world, particularly electroshock, the international arena is important too.
The second theme is there needs to be a consensual organizational structure to coordinate our grass roots efforts.
Currently, society not only tolerates, but actively supports the violation of legal rights through forced psychiatry. I believe this is because of two fundamental factors: 1. People are afraid. 2. They think it is "good for them." Since judges (and governments) are a reflection of the society in which they operate, they condone, if not actively participate in the violations of legal rights.[1] Thus, until society can be educated to understand that forced psychiatry is both harmful to its recipients and does not make them safer, ultimate success will elude us.
Similarly, we must have alternatives to forced psychiatry because by definition we are talking about disturbed and disturbing people. It is unrealistic to expect that people will not be involuntarily committed and forced drugged (or electro-shocked), even when they don't meet the legal requirements, if there is no alternative. Individual cases can be won through large individual efforts, but changing the environment of force requires there to be viable alternatives available.
The legal process may very well establish the right to the "less restrictive alternative" and as a legal matter, the state could not lock people up and force "treat" them if there was a viable less restrictive alternative whether it was actually available or not, but as a practical matter such alternatives need to be available.[2]
Finally, with the recent revelations about the drug companies withholding information about the dangers and lack of efficacy of the Selective Serotonin Re-Uptake Inhibitor (SSRI) anti-depressants, Big Pharma has a moment of vulnerability which must be exploited. This is an historic opportunity that won't last long and it is important to take advantage of it.
The Psycho-Pharmaceutical Complex has literally billions of dollars behind it and we are poor. We have truth and justice on our side. It is not enough. We need to be smart in how we go about it and we need to be unified. The "movement" has a number of differing outlooks on various issues, but it is suggested here that everyone should be able to unite around the issue of human rights in psychiatry, while respecting everyone's right to pursue other, related issues where there might not be agreement. Similarly, there are a number of organizations who share the fundamental value against forced psychiatry which are natural allies.
III. Unifying Principles
It seems to me there are a number of principles that we all ought to be able to agree on.[3] The first and most basic is that people are entitled to freedom, equality and human rights.
We all ought to also be able to agree that psychiatry has and uses abusive power driven by fear and absolution, justified by faulty science, and sustained by lies.[4]
Arising out of this is the principle that people are entitled to the truth. A related principle is that people are entitled to be free of coercive treatment that is based on lies.[5],[6]
IV. Goals
A. Elimination of Forced "Treatment."
Most people, including myself, believe it is unrealistic to think that forced "treatment" will be eliminated completely.[7] Others on "our side" may believe it is warranted in certain circumstances. My view is the goal should be elimination if for no reason other than the system we have now is legally supposed to be used only in the most extreme cases, but in practice many times the number of people who actually legally qualify for forced "treatment" under the current laws are subjected to it.[8] In other words, theoretically legitimate reasons for confinement of a small number of people becomes the unrestrained confinement of a very large number of people who do not meet commitment criteria. As to forced drugging and electroshock, I have a hard time coming up with any legitimate scenarios to employ them. As a practical matter, however, if their use were limited to the actual legal requirements for employing them, I estimate the problem would be reduced by at least 90%.[9]
B. Public Awareness About the Lack of Effectiveness and Extreme Harm of Treatments
The Pharmaceutical Industry, aided and abetted by organized Psychiatry has lied about the effectiveness and safety of psychiatric treatments and the public has accepted these lies as truth. They have no demonstrated effectiveness, particularly long term, and especially if quality of life is considered. These drugs are also extremely harmful -- essentially not only intentionally brain damaging, but with other serious physical toxicities.[10] Not only are they ineffective in the long run, they increase the probability of relapse. In other words, the public thinks they are being protected from the insane by insisting on these medications, but the truth is they are increasing the problem.[11]
As mentioned above, it is my view that the only way to truly achieve a change in the way the legal system works is to destroy the value the public sees in forced psychiatry.
(1) Public Awareness that There is No Evidence Supporting the Broken Brain Theory of Mental Illness
While as a strictly logical matter, challenging the "Medical Model" of mental illness, i.e., the theory that mental illness is the result of a biological defect of some kind in a person's brain, is not necessary to show that the current treatments are neither safe nor effective, in truth, this belief in the medical model is the foundation upon which the drug and electroshock "treatment" is built upon. The Fast for Freedom's (incredibly successful) challenge to the Medical Model understood this dynamic. Unless the Medical Model is debunked, Psychiatry can, as it has for hundreds of years now (since it took over from the exorcists), "discover" miracle "treatments" that are imposed on people with great harm, only to be replaced by the next miracle "treatment" that comes along when it is found out they are ineffective and extremely harmful. Therefore, even though as a strictly logical matter, debunking the Medical Model is not a necessary element, as a practical matter I think it is.[12]
C. Availability of Truly Helpful Alternatives
Unless there are viable alternatives to the current regime for people who are behaving in ways that are frightening to others (and often themselves) I think we are doomed to failure.[13] Thus, the third leg of the stool for human rights in mental health is the availability of truly helpful alternatives. And, if truth be known, even though the "less restrictive alternative" is applicable (i.e., one can't be forced drugged if there is a less restrictive alternative) even if no alternatives are available, as a practical matter they need to be.[14] To be truly helpful, these alternatives must be voluntary and the Soteria experience shows that it is possible.[15]
V. Roots of Psychiatric Power
Perhaps it need not be said because it may be too obvious, but I think it is important for people to understand that I see the effort as a contest, competition -- or even war, if you will -- where our objective is to "win" against the forces of coercive psychiatry.[16] In order to win such a war, it is important to understand our enemy(ies)/opponent(s), their strengths and weaknesses as well as our own.
To me the first question that arises is how did psychiatry come to have so much power that it can have people locked up who have committed no crime and subject them to harmful, brain disabling treatments such as forced drugging and electroshock,[17] which often completely ruin people's lives?
I think the answer is two-fold. First, society has abdicated its responsibility to psychiatry out of fear and the unwillingness to otherwise deal with people whose behavior it finds objectionable. Turning them over to psychiatrists to deal with is easy. Prior to the medicalization of madness, people were considered "possessed" (either divinely or by evil spirits depending on culture and/or behavior). The priests with their religious theories have been replaced by the psychiatrists and their medical theories. Just as the priests had an explanation that fit with the times, psychiatry's Medical Model does so today. The supreme seductiveness, both to the parents of those labeled mentally ill and, often, to their children, of no-fault mental illness is extremely compelling. The Medical Model, while not having scientific support, seems internally consistent, and fits with society's belief system generally. These mechanisms positively reinforces its sway over the public."[18]
Of course, Big Pharma's making literally Billions of Dollars from psychiatric drugs and its (completely rational, if immoral) willingness to spend liberally to protect those profits, including essentially buying off and in support of the psychiatry industry is another root of its power.[19]
VI. Psychiatry’s Strengths
As important as understanding the roots of psychiatry's power is, it is even more important to understand psychiatry's strengths.[20]
Perhaps the most important strength, for all practical purposes, is the unlimited financial resources available to support it, courtesy of Big Pharma.
Another is psychiatrists' stature in society as the presumed experts on "mental illness."[21]
Another is the Psycho-Pharmaceutical Complex's virtual stranglehold on the story presented by the media.[22] Control of the story is hugely important.
Another hugely important source of psychiatry's strength is its alliance with family members as exemplified by NAMI[23] and CHADD.[24] In other words, through its alliance with the parents of people labeled with mental illness, Medical Model Psychiatry has literally positioned itself to be a "motherhood issue."
VII. Psychiatry’s Vulnerabilities
Of course, finding and exploiting coercive psychiatry's vulnerabilities are the keys to prevailing.
Mainstream psychiatry's vulnerabilities include that it is intellectually and morally bankrupt. It's whole claim to authority is based upon it being part of medical science, yet has, as yet failed to produce any valid evidence in support of its claims.[25] The same goes for the validity of its treatments.[26] In other words, it forces people to undergo harmful, ineffective "treatments" through a dishonest legal process.[27]
These are general vulnerabilities, but more recently the pharmaceutical industry has been exposed as jeopardizing people's health and lives on the altar of profits. The industry's concealing data about suicidality from SSRI's and causing heart attacks from Vioxx and the other Cox-2 Inhibitors creates a unique opportunity to press the point about the industry hiding information about the harmfulness and lack of effectiveness of the stronger psychiatric medications.
Another vulnerability is that the cost of all of this psychopharmacology has gotten to the point where policy makers are starting to see it as a problem.[28] Also, a paradigm that unnecessarily creates people who are permanent financial burdens on the government is something the government(s) may finally be willing to look at.
Another vulnerability are the psychiatrists who engage in forced psychiatry, themselves. In my view, people who commit perjury to obtain court orders are not, as a general matter courageous. In fact, I would posit the opposite, and that if they began to see themselves as personally vulnerable to legal liability as a result of their activities many would run for cover.
VIII. Our Strengths
What are the strengths that we bring to this effort?
We are in the right.
We have grass roots support. We potentially have a lot of people who are willing to put in a lot of effort. We have people who are willing to demonstrate and potentially commit civil disobedience to draw attention to our cause. We have allies and potential allies.
Organizations (and their members) that appear perfectly aligned with this effort include:
- MindFreedom/Support Coalition International.[29]
- Law Project for Psychiatric Rights (PsychRights)[30]
- International Center for the Study of Psychiatry and Psychology (ICSPP)[31]
- National Association of Rights Protection and Advocacy (NARPA).[32]
There are no doubt more.[33] In addition there are many C/S/X[34] groups that seem like natural allies and Internet communities with memberships that should be allies. There are also many parents and other family members of people labeled with mental illness that are very much against the current regime.
IX. Our Weaknesses
We have two huge weaknesses: We are as poor as church mice and we don't have an organizational structure that allows us to assign people to tasks.
X. Organizational Structure
We obviously need to raise money and if we raised enough, we could have some paid staff, but as a practical matter, we are composed of volunteers, although some organizations seem likely contribute some staff time, such as MindFreedom, PsychRights and ICSPP.[35] Those contributions are functionally the same as being volunteers though, in the sense that such staff time will only be contributed to the extent it is consistent with the organization's purpose(s).
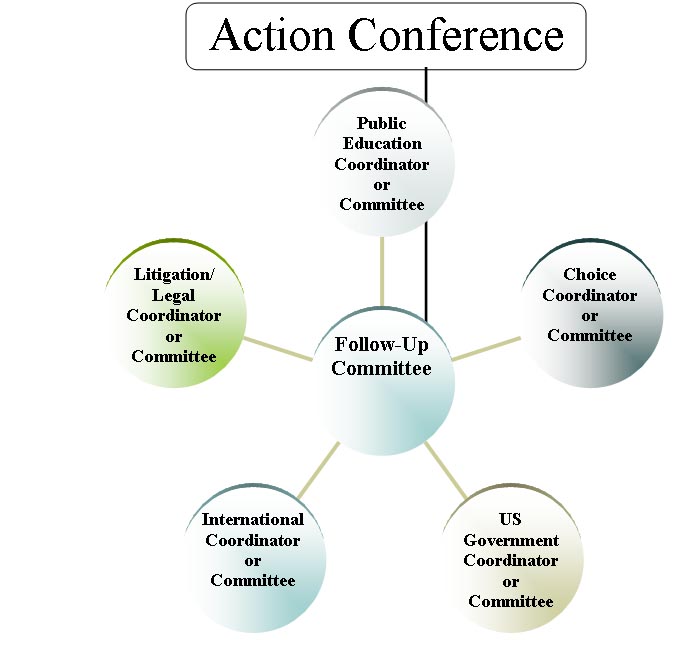
Any organizational structure must recognize this basic fact. Volunteers tend to only do the things they want to do. We need a large number of volunteers and we need to have them used effectively. In other words, it is a (hopefully) huge volunteer management effort. The key features are to keep track of tasks that have been identified to be accomplished, match them with volunteers, keep track of results, etc. This needs to be part of some sort of overall organizational structure. The Action Conference, which prompted this paper is designed to come up with specific actions to be taken and people who sign up to work on them. These need to be kept track of and the effort needs to be managed as things go forward.[36] Even though the Action Conference is a bottom up effort in designing the agenda, in order to be effective, the effort needs to be coordinated.
This requires a structure. The Action Conference Tracks can be thought of as "Spheres of Action" with a person or committee charged with following up on the Action Conference agenda for that sphere and all of them joining together as a Follow-up Committee that would coordinate things between action conferences. Ideally, we would have an action conference annually to set/adjust the action agenda.[37] The following diagram hopefully captures the idea: