| HOME | SEARCH | CURRENT ISSUE | PAST ISSUES | COLLECTIONS | HELP |
|
|
|
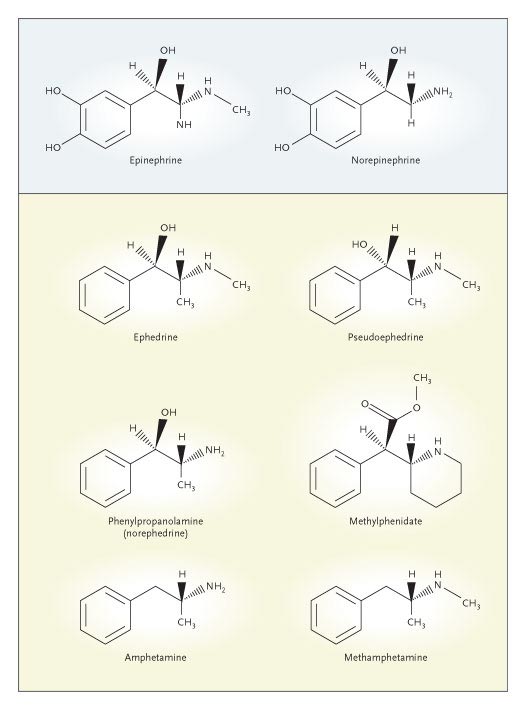
The drugs under review were primarily amphetamines (Adderall and other brands) and methylphenidate (Ritalin, Concerta, and other brands). These agents are closely related members of the class of sympathomimetic amines, the structures of several of which are shown in the diagram. These compounds exert potent stimulant effects on the cardiovascular and central nervous systems. One of the oldest such agents, methamphetamine, was originally synthesized in 1891 and first widely used during World War II in Nazi Germany to enhance the ability of Luftwaffe pilots to stay alert during extended hours of combat. Medical use of this agent is now limited, but illicit use has grown rapidly and now represents an increasing public health problem. When smoked or injected intravenously, methamphetamine ("speed") is associated with hyperthermia, rhabdomyolysis, myocardial infarction, stroke, and sudden death — effects well known to coroners in regions of the United States where abuse is common. Beginning in the 1950s, the stereoisomer dextroamphetamine and related agents were introduced as appetite suppressants.
|
The concern of the advisory committee reflected several considerations. The cardiovascular effects of the sympathomimetic amines have been thoroughly described in the medical literature. These agents substantially increase the heart rate and blood pressure. In a placebo-controlled trial, mixed amphetamine salts (Adderall) administered to adults increased systolic blood pressure by about 5 mm Hg; similar effects were found with methylphenidate formulations.2 Blood-pressure changes of this magnitude, particularly during long-term therapy, are known to increase morbidity and mortality. In 2005, a separate FDA advisory committee that I chaired concluded that blood-pressure changes represented such a reliable predictor of cardiovascular outcomes that class labeling would be appropriate in most cases.3 The increases in heart rate induced by sympathomimetic agents also have well-described adverse cardiovascular effects. The administration of these drugs produces persistent increases in heart rate, inducing chronic heart failure in animal models of dilated cardiomyopathy.
A review of the regulatory history of this class of drugs also helps to explain why the advisory committee took decisive action. The dietary supplement ephedra, sometimes called ma huang, contains two alkaloids, ephedrine (see diagram) and its enantiomer, pseudoephedrine. These supplements have been used by millions of Americans to assist in weight loss or to increase energy. Some athletes have advocated the use of ephedra-containing dietary supplements as performance-enhancing agents. On December 31, 2003, federal officials announced plans to ban ephedra immediately. Health and Human Services Secretary Tommy Thompson told reporters, "The time to stop using these products is now." This action followed several high-profile catastrophic outcomes linked to ephedra products, including the death of 23-year-old Baltimore Orioles pitcher Steve Bechler. Published studies reported that sales of ephedra-containing supplements represented less than 1 percent of all dietary-supplement sales but that these products accounted for 64 percent of the serious adverse reactions to supplements reported to the Centers for Disease Control and Prevention.4 Unfortunately, in April 2005, a federal court in Utah struck down the federal ban on ephedra. Many companies that make these products are located in Utah.
Similar regulatory actions have been proposed for phenylpropanolamine (PPA), another closely related sympathomimetic amine (see diagram). On December 22, 2005, the FDA issued a notice of "proposed rulemaking for over-the-counter nasal decongestant and weight control products" containing PPA. The notice called for a public comment period until March 22, 2006, after which the FDA would undertake regulatory action that would probably include banning the use of the agent in over-the-counter preparations. The FDA's action followed many years of concern about the potential of PPA products to cause hemorrhagic stroke. Six years ago, a case–control study published in the Journal reported a 16-fold increase in the risk of stroke among women taking PPA for appetite suppression.5
Briefing documents prepared for the February 9 advisory-committee meeting described cases of myocardial infarction, stroke, and sudden death in children and adults taking ADHD stimulants.1 These narratives were derived from the FDA's Adverse Event Reporting System (AERS), a database containing reports of adverse events submitted by health care providers. The AERS is a voluntary reporting system that has been criticized because only 1 to 10 percent of serious adverse events are actually reported, limiting the database's usefulness for identifying emerging drug hazards. The drug-related events reviewed by the committee included 25 cases of sudden death in children or adults (see table), some with evidence on autopsy of undiagnosed congenital heart disease, such as hypertrophic obstructive cardiomyopathy. The physiology of this condition renders patients particularly vulnerable to the adverse effects of sympathomimetic drugs, because such agents increase contractility, thereby increasing the pressure gradient in the left ventricular outflow tract. Many additional cases of major adverse cardiovascular events, including myocardial infarction, stroke, and serious arrhythmias, were reviewed by the committee. However, the documentation of cases was frequently incomplete, and neither the FDA reviewers nor the committee considered the AERS data to be definitive.
|
Source Information
Dr. Nissen is the interim chairman of the Department of Cardiovascular Medicine at the Cleveland Clinic, Cleveland, and was a consultant to the FDA's Drug Safety and Risk Management Advisory Committee for the hearings on ADHD drugs.
This article was published at www.nejm.org on March 20, 2006.
An interview with Dr. Nissen can be heard at www.nejm.org.
References
| |||||||||||||||||||||||||||||||||||||||||||||
This article has been cited by other articles:
HOME | SEARCH | CURRENT ISSUE | PAST ISSUES | COLLECTIONS | HELP Comments and questions? Please contact us. The New England Journal of Medicine is owned, published, and copyrighted © 2006 Massachusetts Medical Society. All rights reserved. |