By ANNA WILDE MATHEWS
Gage Martindale, who is 8 years old, has been taking a blood-pressure drug since he was a toddler. "I want to be healthy, and I don't want things in my heart to go wrong," he says.
And, of course, his mom is always there to check Gage's blood pressure regularly with a home monitor, and to make sure the second-grader doesn't skip a dose of his once-a-day enalapril.
These days, the medicine cabinet is truly a family affair. More than a quarter of U.S. kids and teens are taking a medication on a chronic basis, according to Medco Health Solutions Inc., the biggest U.S. pharmacy-benefit manager with around 65 million members. Nearly 7% are on two or more such drugs, based on the company's database figures for 2009.
Doctors and parents warn that prescribing medications to children can be problematic. There is limited research available about many drugs' effects in kids. And health-care providers and families need to be vigilant to assess the medicines' impact, both intended and not. Although the effects of some medications, like cholesterol-lowering statins, have been extensively researched in adults, the consequences of using such drugs for the bulk of a patient's lifespan are little understood.
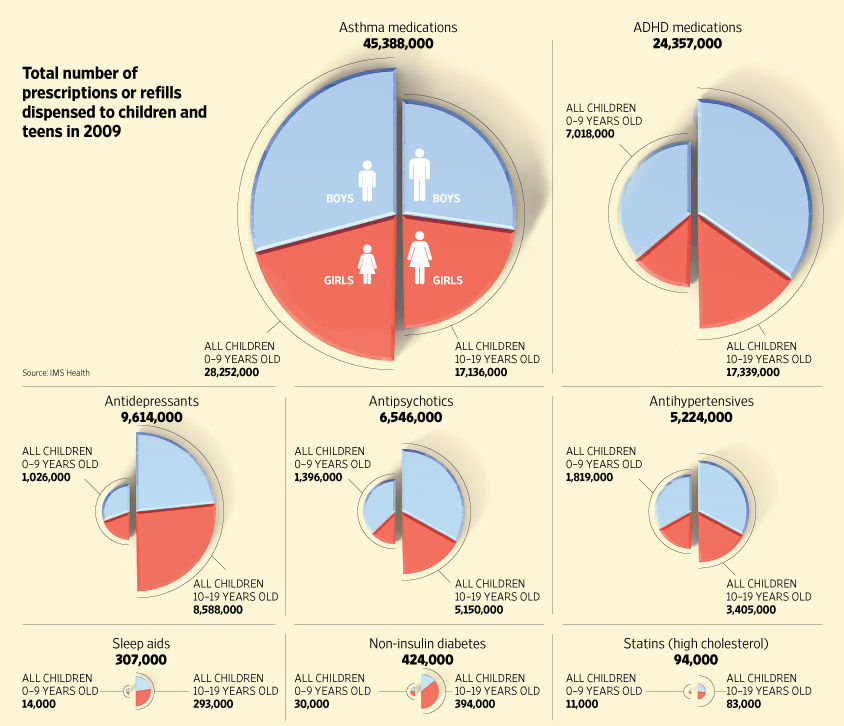
Many medications kids take on a regular basis are well known, including treatments for asthma and attention-deficit hyperactivity disorder.
But children and teens are also taking a wide variety of other medications once considered only to be for adults, from statins to diabetes pills and sleep drugs, according to figures provided to The Wall Street Journal by IMS Health, a research firm. Prescriptions for antihypertensives in people age 19 and younger could hit 5.5 million this year if the trend though September continues, according to IMS. That would be up 17% from 2007, the earliest year available.
Researchers attribute the wide usage in part to doctors and parents becoming more aware of drugs as an option for kids. Unhealthy diets and lack of exercise among children, which lead to too much weight gain and obesity, also fuel the use of some treatments, such as those for hypertension. And some conditions are likely caught and treated earlier as screening and diagnosis efforts improve.
Gage, who isn't overweight, has been on hypertension drugs since he had surgery to fix a heart defect as a toddler, says his mother, Stefanie Martindale, a Conway, Ark., marketing-company manager.
Most medications that could be prescribed to children on a chronic basis haven't been tested specifically in kids, says Danny Benjamin, a Duke University pediatrics professor. And older drugs rarely get examined, since pharmaceutical firms have little incentive to test medicines once they are no longer under patent protection.
Still, a growing number of studies have been done under a Food and Drug Administration program that rewards drug companies for testing medications in children. In more than a third of these studies, there have been surprising side effects, or results that suggested a smaller or larger dose was needed than had been expected, Dr. Benjamin says. Those findings underscore that children's reactions to medicines can be very different than those of adults. Long-term effects of drugs in kids are almost never known, since pediatric studies, like those in adults, tend to be relatively short.
"We know we're making errors in dosing and safety," says Dr. Benjamin, who is leading a new National Institutes of Health initiative to study drugs in children. He suggests that parents should do as much research as they can to understand the evidence for the medicine, confirm the diagnosis, and identify side effects. Among the places to check: drug labels and other resources on the FDA's website, published research at www.pubmed.gov, and clinical guidelines from groups like the American Academy of Pediatrics.
When a child psychiatrist diagnosed their then 8-year-old daughter with bipolar disorder four years ago, Ken and Joy Lewis, of Chapel Hill, N.C., sought a second opinion from another child psychiatrist.
They also worked with a psychologist. Dr. Lewis, who leads a company that does early-stage drug studies, reads all the available research on each medication suggested for the girl, now 12, who has taken antipsychotics and other psychiatric medications including Risperdal and Haldol.
"If your child has a chronic problem, then you have to invest the time as a parent," he says.
Parents and doctors also say nondrug alternatives should be explored where possible. Tom Wells, a professor of pediatrics at the University of Arkansas for Medical Sciences who sees patients at Arkansas Children's Hospital in Little Rock, frequently pushes diet and exercise changes before drugs for hypertensive kids. "Obesity is really the biggest cause I see for high blood pressure in adolescents," he says. But only about 10% of families adhere to his diet and exercise recommendations, he says.
Beverly Pizzano, a psychologist who lives in Palm Harbor, Fla., spent years struggling with behavioral therapies for her son Steven, 10, who showed symptoms of ADHD at a young age. She worked with a counselor on a system of rewards for good behavior, and even had a research team watch him and suggest interventions. But she turned to medications after he struggled in kindergarten. "We tried everything before I would get to that," she says.
After a drug is prescribed, children must be closely monitored, doctors say. They may not recognize or communicate a possible side effect, or whether their symptoms are improving. They also don't always follow prescription instructions.
Robert Lemanske, a professor at the University of Wisconsin in Madison, says patients at his pediatric asthma clinic are checked regularly for side effects such as slowed rates of growth. He quizzes parents and young patients on details like where they keep their inhalers to make sure they're taking their prescribed medicine.
Nichole Ramsey, a preschool teacher whose 9-year-old son Antwone is a patient at the clinic, watches her son's basketball practices so she can head off any wheezing or other symptoms. She also makes sure she's around when he gets his regular Advair dose. If Antwone stays at a friend's house overnight, she asks the parents to watch that he takes steps like rinsing out his mouth to avoid a fungal infection that can be a side effect of the inhaled drug.
"You're still the best monitor of what's going on with them," she says of a parent's role.
Ms. Ramsey is particularly concerned about Advair, which has been tied to rare instances of asthma-related death, but says it works better than a previous drug he was using. Before he started the medications, Antwone was hospitalized several times for asthma attacks.
As children's bodies change and grow, they often need different drugs or doses, says Greg Kearns, chairman of medical research at Children's Mercy Hospital in Kansas City, Mo.
Jennifer Flory, a homemaker in Baldwin City, Kan., says that after her daughter Cassandra, now 16, started taking a higher dose of the asthma drug Singulair a few years ago, she became more moody and sad. Ms. Flory didn't connect the change to the drug, but when she eventually mentioned it to a nurse practitioner at the girl's asthma clinic, the nurse suggested stopping Singulair, which currently has a precaution in its label about possible psychiatric side effects. Cassandra, who continued taking Advair, became far more cheerful and didn't have any increase in asthma symptoms, Ms. Flory says.
A spokesman for Merck & Co., which makes Singulair, said in a statement that the company is "confident in the efficacy and safety of Singulair," which is "an important treatment option for appropriate patients."
Write to Anna Wilde Mathews at anna.mathews@wsj.com







![[0924grubel01]](./101228WSJSoYoungSoManyPills_files/OB-PU630_0924gr_A_20110924080355.jpg)
![[pinker]](./101228WSJSoYoungSoManyPills_files/OB-PU572_pinker_A_20110923180338.jpg)
![[0924putin01]](./101228WSJSoYoungSoManyPills_files/OB-PU622_0924pu_A_20110924064015.jpg)
![[PIGS]](./101228WSJSoYoungSoManyPills_files/NA-BN439_PIGS_C_20110923184437.jpg)
![[BEATLES4]](./101228WSJSoYoungSoManyPills_files/RV-AE383_BEATLE_C_20110923190026.jpg)
![[GOLF]](./101228WSJSoYoungSoManyPills_files/WO-AH132B_GOLF_C_20110923230933.jpg)
![[BERLUSCONI]](./101228WSJSoYoungSoManyPills_files/RV-AE379_BERLUS_C_20110923033505.jpg)






Most Recommended
“Forcing communities to actively...;”
“The Marxist view is that anybody...;”
“This is the same Ms. Noonan who...;”
“Soooooooooo... We have Buffett...;”
“Europe will become one unified...;”